Insilico Medicine just moved rentosertib, a drug whose biological target was identified by AI and whose molecule was designed by generative AI, into a Phase III clinical trial with 320 patients across 47 centers in China. If you build tools for drug discovery, this is the most important clinical milestone in AI-originated therapeutics to date, because it is the first time a molecule born from a generative chemistry engine has cleared Phase II and entered pivotal late-stage testing. The Phase IIa results, published in Nature Medicine in 2025, showed a +98.4 mL mean forced vital capacity improvement in the 60 mg once-daily arm versus a 20.3 mL decline in placebo over 12 weeks. That signal was strong enough to justify a full Phase III program measuring annual FVC decline over 52 weeks. The trial initiated on July 7, 2026, according to Insilico's announcement from Cambridge, Massachusetts.
This is the first fully AI-originated drug to reach Phase III, and the data trail behind it is unusually deep.
What exactly did Insilico's AI pipeline produce?
The rentosertib program ran through Insilico's Pharma.AI platform, which splits the drug discovery process into two distinct computational engines. PandaOmics, the biology engine, ingested multi-omics data from fibrotic tissues, clinical trial outcomes, academic literature, and patent intelligence to build biological network models. It then applied causal inference to rank potential drug targets, scoring them on their connection to aging-related disease mechanisms. PandaOmics identified TNIK (TRAF2- and NCK-interacting kinase) as the top candidate in the protein and receptor kinase category, a target that existing antifibrotic drugs do not address. The existing IPF therapies, nintedibib and pirfenidone, target receptor tyrosine kinase pathways. TNIK sits upstream of multiple fibrosis-driving signaling channels: Wnt, TGF-beta, Hippo/YAP-TAZ, JNK, and NF-kappaB.
Once the target was selected, Chemistry42 took over. Rather than screening existing compound libraries, the generative chemistry engine used Generative Tensorial Reinforcement Learning to design molecules that fit the TNIK protein pocket. The system synthesized 79 physical molecules for testing and selected the 55th iteration as the preclinical candidate. The timeline from project initiation to preclinical candidate nomination was 18 months, a fraction of the traditional pharmaceutical discovery timeline that typically spans several years and thousands of compounds.
The full discovery-to-clinic journey was published in Nature Biotechnology, the medicinal chemistry in the Journal of Medicinal Chemistry, and the Phase IIa clinical results in Nature Medicine. The FDA granted Orphan Drug Designation to rentosertib for IPF in February 2023.
How convincing was the Phase IIa data?
The GENESIS-IPF Phase IIa trial was a multicenter, double-blind, randomized, placebo-controlled study that enrolled 71 patients across 22 sites in China. Patients were randomized to placebo, 30 mg once daily, 30 mg twice daily, or 60 mg once daily, for 12 weeks.
The trial met its primary safety and tolerability objective. Treatment-emergent adverse event rates were similar across all arms. On the efficacy side, the signal was dose-dependent and clinically notable: the 60 mg once-daily arm showed a mean FVC change of +98.4 mL at 12 weeks, compared with a mean decline of 20.3 mL in the placebo group. That is a spread of nearly 119 mL between active treatment and placebo in a disease where lung function progressively deteriorates.
For context, IPF is a progressive fibrotic lung disease with a median survival of two to four years after diagnosis. The two approved antifibrotic therapies, nintedibib and pirfenidone, slow progression but do not halt or reverse it. A drug that actually improves FVC rather than merely slowing its decline would represent a mechanistic leap, which is exactly what the Phase III trial is designed to confirm.
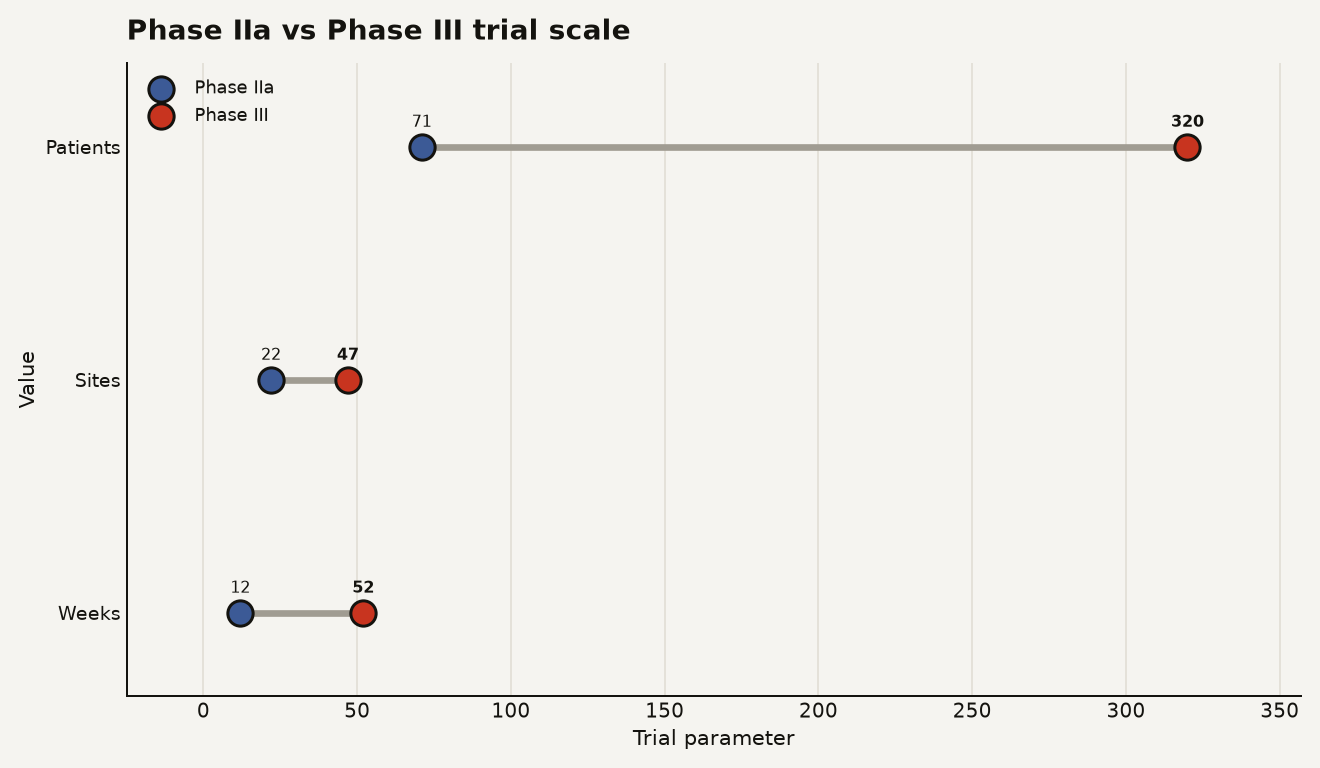
The chart above shows the scale-up from Phase IIa to Phase III: 71 to 320 patients, 22 to 47 sites, and 12 to 52 weeks of treatment. The primary endpoint shifts from safety and tolerability to the annual rate of FVC decline, with a key secondary endpoint of time to first disease progression event.
Why should builders in AI drug discovery care about this specific trial?
The rentosertib program matters for three reasons that go beyond the clinical result itself.
First, it is the most complete documented proof that an AI pipeline can originate a novel target and a novel molecule and advance it through human trials. Plenty of AI drug discovery companies have produced preclinical candidates or early Phase I data. Insilico has now published the full arc in peer-reviewed journals, from computational target selection through generative chemistry, preclinical pharmacology, Phase I safety, randomized Phase IIa efficacy, and into Phase III. If you are building computational drug discovery tools and your investors or partners ask whether AI-originated drugs can reach late-stage trials, this is your reference case.
Second, the economics of the generative chemistry approach look different from traditional high-throughput screening. Synthesizing 79 molecules and advancing the 55th is a radically compressed funnel compared with the industry standard of screening tens of thousands of compounds. The 18-month timeline from project initiation to preclinical candidate is the kind of number that changes how biopharma teams think about resource allocation. A team that previously budgeted three to five years for lead identification now has a documented case where generative chemistry did it in under two years.
Third, the proteomic biomarker strategy embedded in the trial is worth studying. Insilico deployed internal proteomic aging clocks, including ProtAge, OrganAge, ipfP3GPT, and PAOPAC, to track predicted biological-age changes from the intervention. They used UK Biobank age-associated trajectories as external comparison data. This is a different kind of clinical readout than standard endpoints, and it reflects a growing interest in how AI-driven proteomics can supplement traditional clinical measures.
Here is what this means for you concretely:
- If you build target discovery tools, PandaOmics' approach of integrating multi-omics data with aging-relevant scoring and causal inference is now a validated template, not a theoretical one. TNIK was an underexplored target that computational prioritization surfaced.
- If you build generative chemistry platforms, Chemistry42's synthesis of only 79 physical molecules to reach a clinical candidate sets a benchmark for molecular generation efficiency that you should measure against.
- If you are evaluating AI drug discovery companies, the question is no longer whether AI can produce clinical candidates. The question is whether their Phase III data will hold. Rentosertib's 12-week FVC signal needs to survive a 52-week, 320-patient trial.
- If you are in business development, Insilico also signed a $600 million deal with Takeda in July 2026, signaling that large pharma is willing to pay for AI-discovered programs that have cleared Phase II.
What are the risks and open questions heading into Phase III?
The Phase III trial carries several risks that the Phase IIa data cannot resolve.
The Phase IIa study was small. Seventy-one patients across four arms means roughly 18 patients per arm, which is standard for a safety trial but underpowered for efficacy conclusions. The +98.4 mL FVC improvement in the 60 mg arm is a promising signal, but it came from a 12-week observation window. The Phase III primary endpoint measures annual rate of FVC decline over 52 weeks, a fundamentally different question: can the drug sustain its effect over a full year in a larger population?
The trial is also entirely in China. All 47 centers are Chinese clinical sites, and the principal investigators are from Peking Union Medical College Hospital and Shanghai Pulmonary Hospital. That design decision makes sense given Insilico's operational base and the prevalence of IPF in the region, but it raises questions about whether the data package will satisfy regulators in the United States and Europe without bridging studies. The FDA's Orphan Drug Designation gives the program certain incentives, including tax credits and market exclusivity, but it does not constitute approval.
The competitive landscape also matters. Existing antifibrotic therapies generated combined sales exceeding $3 billion annually before generic competition eroded pricing. A disease-modifying therapy that actually improves lung function rather than slowing decline would command a premium, but only if the Phase III data replicates the Phase IIa signal.
There is also a scientific question about the senomorphic angle. Research published in Aging and Disease showed that TNIK inhibition produces senomorphic activity, reducing extracellular matrix remodeling markers in cellular senescence models. Insilico's CSO, Feng Ren, framed IPF as a disease where fibrosis, chronic inflammation, and cellular senescence intersect. The Phase III trial is not designed to test the senescence hypothesis directly, but the proteomic aging clock data collected alongside the primary endpoint could provide supporting evidence if the clinical result is positive.
What this trial really tests
The rentosertib Phase III trial is the first time a generative AI pipeline faces the definitive test of clinical efficacy at scale. The discovery was fast, the molecule was novel, the target was computationally prioritized, and the Phase IIa signal was real. Now 320 patients over 52 weeks will determine whether AI drug discovery has produced a medicine or a milestone. The distinction matters.
Sources
- Insilico Medicine announcing the Phase III trial initiation for rentosertib on July 7, 2026
- Nature Medicine publishing the Phase IIa GENESIS-IPF trial results
- Nature Biotechnology publishing the discovery-to-clinic progression of the TNIK inhibitor
- PR Newswire distributing Insilico's Phase III announcement
- AI News reporting on the Phase III advancement and computational pipeline details